
If you've noticed subtle darkening around your cheeks, forehead, or upper lip despite your best skincare efforts, you're experiencing what dermatologists call the 'pigmentation paradox'—the frustrating reality that hyperpigmentation is far easier to prevent than to treat. Understanding this changes everything about how you approach your daily skincare routine. Here's what makes prevention so powerful: melanocytes, the cells that produce pigment, can be triggered by UV exposure, inflammation, hormonal changes, and even heat. Once activated, they can remain hypersensitive for months or years, creating persistent dark spots that resist even aggressive treatment. But when you prevent that initial trigger, you bypass this entire cascade—keeping melanocytes calm and your skin tone even. In Australia's intense UV environment, where UV Index readings regularly exceed 10 during summer months, prevention strategies need to be comprehensive and consistent. This isn't about occasional sunscreen application; it's about building a multi-layered defence system that addresses every pathway to pigmentation development. Here's exactly how to protect your skin from the invisible triggers that create tomorrow's dark spots.
Why Does Hyperpigmentation Prevention Matter More Than Treatment?
The science behind pigmentation reveals a crucial insight: prevention works at the cellular level before visible damage appears, whilst treatment attempts to reverse changes that have already altered your skin's melanin production patterns.
When UV radiation, inflammation, or hormonal signals activate melanocytes, they trigger a complex cascade involving tyrosinase enzyme activation, melanin synthesis, and melanin transfer to surrounding skin cells. This process creates not just immediate darkening, but also 'melanocyte memory'—a phenomenon where pigment-producing cells remain hyperresponsive to triggers for extended periods. Research by Ortonne and Bissett (2008) demonstrates that melanocytes can stay activated for 6-12 months after a single inflammatory event, explaining why post-inflammatory hyperpigmentation persists long after the initial trigger resolves.
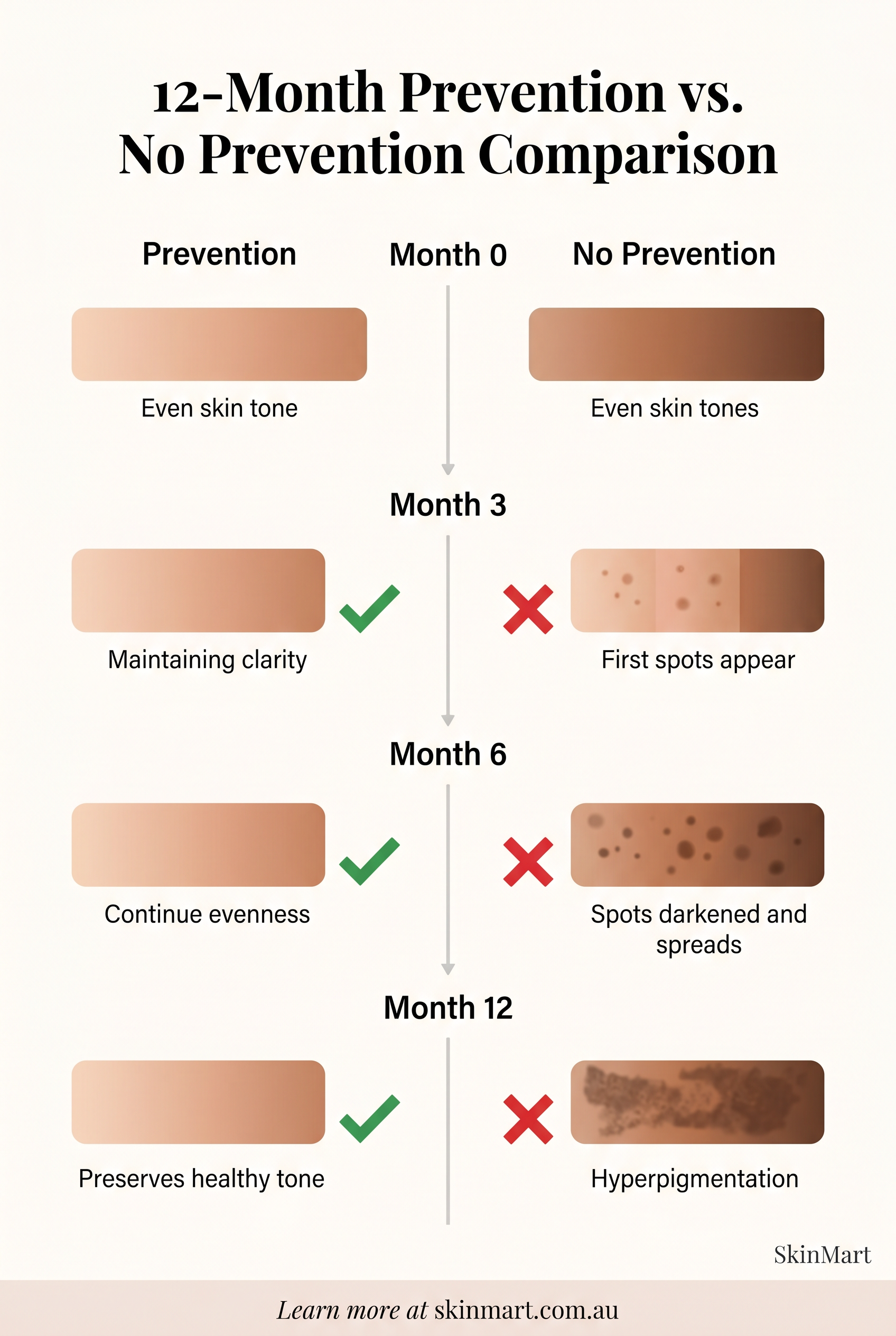
Prevention interrupts this cascade before it begins. By blocking UV radiation, neutralising inflammatory mediators, and supporting barrier function, you prevent melanocyte activation entirely. This approach is exponentially more effective than attempting to inhibit tyrosinase or accelerate melanin degradation after pigmentation has already formed. The clinical evidence is compelling: studies show that consistent broad-spectrum photoprotection reduces hyperpigmentation incidence by 80-90%, whilst treatment of existing pigmentation achieves 40-60% improvement over similar timeframes (Sheth & Pandya, 2011).
For Australian skin facing year-round high UV exposure, this prevention-first approach becomes even more critical. The cumulative UV dose in Brisbane or Sydney far exceeds that of many global regions, creating accelerated pigmentation risk that makes reactive treatment strategies perpetually inadequate.
What Are the Complete Photoprotection Requirements for Pigmentation Prevention?

Comprehensive photoprotection extends far beyond basic SPF application. Understanding the full spectrum of light-induced pigmentation reveals why traditional sun protection often falls short.
UV radiation remains the primary trigger, but visible light—particularly blue light wavelengths (400-500nm)—also stimulates melanogenesis, especially in Fitzpatrick skin types III-VI. Research by Mahmoud et al. (2010) demonstrates that visible light exposure creates persistent hyperpigmentation in darker skin tones through oxidative stress pathways distinct from UV damage. This explains why people with diligent SPF habits still develop melasma and uneven tone—their protection strategy doesn't address the complete light spectrum.
Your prevention strategy requires multi-level photoprotection:
Broad-Spectrum UV Filters: SPF 50+ providing both UVB and UVA protection is non-negotiable in Australian conditions. Physical filters like zinc oxide (20-25%) offer the most comprehensive UV blocking, whilst chemical filters like avobenzone and tinosorb provide elegant cosmetic finish. The key is daily application of 2mg/cm² (approximately ¼ teaspoon for face) with reapplication every 2 hours during sun exposure.
Iron Oxide Inclusion: These mineral pigments (CI 77491, 77492, 77499) provide critical visible light and blue light attenuation that UV filters alone cannot achieve. Studies show iron oxide-enhanced sunscreens reduce melasma recurrence by 40% compared to UV-only protection (Boukari et al., 2015). Look for tinted formulations or add mineral makeup containing iron oxides over your sunscreen.
Antioxidant Enhancement: Topical antioxidants work synergistically with sunscreens by neutralising the oxidative stress that drives melanogenesis. L-ascorbic acid (10-20%), vitamin E (1-5%), and ferulic acid (0.5%) create what researchers call 'antioxidant photoprotection'—reducing UV-induced pigmentation by up to 60% when combined with sunscreen (Lin et al., 2005). Application under sunscreen maximises effectiveness.
Infrared Protection: Australia's intense heat creates significant infrared radiation exposure that generates oxidative stress and triggers inflammatory pigmentation. Antioxidants like green tea polyphenols and niacinamide provide thermal protection, whilst physical barriers (hats, shade-seeking) reduce direct IR exposure.
Key Takeaways
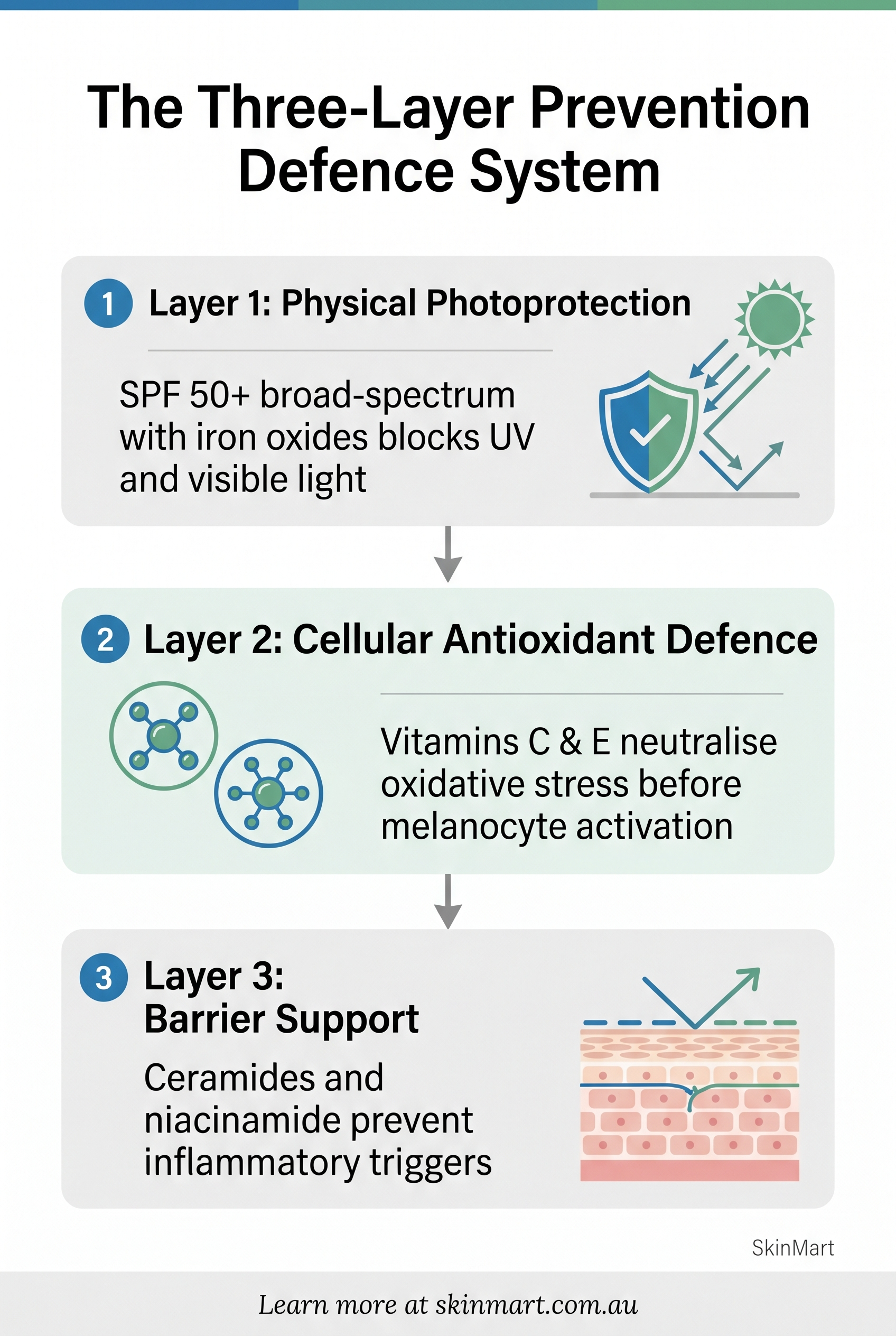
- Hyperpigmentation prevention requires comprehensive photoprotection combining broad-spectrum SPF 50+ with iron oxides for visible light protection, daily antioxidant serums to neutralise oxidative stress, and gentle exfoliation to maintain even cell turnover.
- In Australia's intense UV environment, prevention strategies must address UV, blue light, and infrared radiation whilst supporting your skin's natural barrier function.
- The most effective approach combines physical sun blocking, cellular...
How Do You Build Cellular Defence Against Pigmentation Triggers?
Beyond external photoprotection, prevention strategies must address the cellular mechanisms that translate triggers into visible pigmentation. This requires understanding how to support your skin's natural defence systems whilst neutralising inflammatory pathways.
Antioxidant systems form your first line of cellular defence. When UV radiation or inflammation generates reactive oxygen species (ROS), these unstable molecules trigger the inflammatory cascade that activates melanocytes. Topical and dietary antioxidants neutralise ROS before they can initiate this cascade. The most effective approach combines multiple antioxidants with complementary mechanisms:
Vitamin C (L-Ascorbic Acid): Beyond its direct tyrosinase inhibition, vitamin C neutralises singlet oxygen and superoxide radicals whilst regenerating vitamin E. Clinical studies show 10-20% L-ascorbic acid formulations reduce UV-induced erythema and pigmentation by 40-60% when used consistently (Pinnell et al., 2001). Application should occur in the morning before photoprotection for maximum preventive benefit.
Niacinamide: This versatile active prevents melanosome transfer from melanocytes to keratinocytes—the process that creates visible darkening. Research demonstrates 4-5% niacinamide reduces pigmentation whilst improving barrier function and reducing inflammation (Hakozaki et al., 2002). Its anti-inflammatory properties make it particularly valuable for preventing post-inflammatory hyperpigmentation.
Alpha-Tocopherol (Vitamin E): Working synergistically with vitamin C, vitamin E provides lipid-soluble antioxidant protection and enhances photoprotection effectiveness. The combination of C and E creates more comprehensive ROS neutralisation than either alone.
Barrier function support represents the second critical defence layer. Compromised skin barriers trigger inflammatory responses that activate melanocytes, explaining why irritation, dryness, and sensitisation often precede pigmentation development. Ceramide-based moisturisers, fatty acid supplements, and gentle cleansing preserve barrier integrity, reducing inflammation-driven pigmentation risk.
Gentle exfoliation maintains even cellular turnover without triggering inflammatory pigmentation. Low-concentration AHAs (5-8% glycolic or lactic acid) or PHAs (polyhydroxy acids) prevent the uneven keratinisation that can exacerbate pigmentation appearance whilst avoiding the irritation that triggers new pigment production.
What Lifestyle Modifications Prevent Pigmentation Development?

Daily habits and environmental exposures significantly influence pigmentation risk, often in ways that skincare alone cannot address. Understanding these factors allows you to create comprehensive prevention strategies that extend beyond topical products.
Heat exposure activates melanocytes through inflammatory pathways independent of UV radiation. This explains why melasma often worsens during summer months even with diligent sun protection—the thermal stress itself triggers pigmentation. Practical modifications include seeking shade during peak heat hours (10am-3pm), using cooling facial mists, and avoiding hot yoga or saunas during active pigmentation risk periods.
Hormonal influences, particularly oestrogen fluctuations, dramatically increase melanocyte sensitivity to all triggers. Women using hormonal contraception, pregnant, or perimenopausal face heightened pigmentation risk requiring enhanced prevention strategies. This doesn't mean avoiding hormonal medications, but rather recognising the need for more aggressive photoprotection and anti-inflammatory skincare during these periods.
Inflammatory triggers from aggressive treatments, harsh products, or skin picking create post-inflammatory hyperpigmentation (PIH) that can persist for months. The prevention approach involves:
Treatment Timing: Schedule potentially irritating treatments (chemical peels, laser, aggressive retinoids) during low-UV months (May-August in Australia) when melanocyte activity naturally decreases.
Gentle Product Introduction: New actives should be introduced gradually with careful monitoring for irritation. Redness, stinging, or flaking signal inflammation that may trigger pigmentation in susceptible skin.
Inflammation Management: At the first sign of irritation, reduce active ingredients and increase barrier support. Anti-inflammatory ingredients like centella asiatica, liquorice root extract, and colloidal oatmeal calm reactive skin before pigmentation develops.
Dietary antioxidants provide systemic protection that complements topical strategies. Polyphenol-rich foods (green tea, berries, dark chocolate), carotenoids (carrots, sweet potato, tomatoes), and omega-3 fatty acids reduce systemic inflammation and enhance photoprotection from within. Whilst not replacement for topical protection, dietary antioxidants create foundational cellular defence against oxidative stress.
How Do You Create a Personalised Prevention Strategy for Australian Conditions?
Generic prevention advice fails because pigmentation risk varies dramatically based on individual factors: skin phototype, genetic predisposition, hormonal status, geographic location, and lifestyle sun exposure patterns. Effective prevention requires personalised strategies that account for your unique risk profile.
Skin phototype fundamentally influences both pigmentation risk and optimal prevention approach. Fitzpatrick types I-II face primary risk from UV-induced damage and require aggressive broad-spectrum protection with emphasis on UV filters. Types III-VI experience greater risk from visible light, heat, and inflammatory triggers, necessitating iron oxide inclusion, thermal protection, and anti-inflammatory strategies.
Geographic UV intensity determines baseline photoprotection requirements. Brisbane's average UV Index of 8-12 during summer (reaching 14+ on peak days) demands SPF 50+ with 2-hour reapplication during outdoor exposure. Even winter months maintain UV Index 3-5, requiring daily broad-spectrum protection year-round—a reality that differs significantly from temperate climates where winter photoprotection can be reduced.
Lifestyle exposure patterns reveal hidden pigmentation triggers. Office workers with window exposure accumulate significant UVA and visible light damage through glass. Outdoor exercisers face combined UV, heat, and sweat-induced barrier compromise. Drivers experience asymmetric UV exposure on the window side. Your prevention strategy must address these specific exposure patterns:
High Outdoor Exposure: SPF 50+ mineral formulation with iron oxides, applied 20 minutes before exposure and reapplied every 90-120 minutes. Wide-brimmed hat, UV-protective clothing, and shade-seeking during peak UV hours. Post-exposure antioxidant application to neutralise accumulated oxidative stress.
Moderate Indoor-Outdoor Transition: Daily broad-spectrum SPF 30-50 with iron oxides, morning antioxidant serum, barrier-supporting moisturiser. Enhanced protection (hat, reapplication) during outdoor lunch breaks or commutes.
Predominantly Indoor with Window Exposure: Tinted SPF 30+ with iron oxides for visible light protection, antioxidant serum, blue light consideration for extensive screen time. Window film installation for home office spaces with significant sun exposure.
Hormonal status assessment identifies periods of heightened melanocyte sensitivity requiring enhanced prevention. Pregnancy, hormonal contraception initiation, and perimenopause all increase melasma risk, warranting proactive strategy intensification before pigmentation appears.
What Does an Effective Daily Prevention Routine Look Like?

Translating prevention science into consistent daily practice requires a streamlined routine that integrates multiple protective mechanisms without overwhelming complexity. Here's the evidence-based framework:
Morning Prevention Protocol:
1. Gentle Cleanse: Low-pH, non-stripping cleanser preserves barrier function and prevents inflammatory triggers. Avoid hot water which increases thermal melanocyte activation.
2. Antioxidant Defence: 10-20% L-ascorbic acid serum or stable vitamin C derivative, allowed to absorb for 60-90 seconds. This creates cellular protection against UV-generated oxidative stress.
3. Additional Actives: Niacinamide 4-5% (can be layered with vitamin C despite outdated concerns) provides melanin transfer inhibition and anti-inflammatory benefits. Tranexamic acid 2-5% offers additional tyrosinase inhibition for high-risk individuals.
4. Barrier Support: Lightweight moisturiser with ceramides, niacinamide, or centella asiatica maintains barrier integrity and reduces inflammatory sensitivity.
5. Comprehensive Photoprotection: Broad-spectrum SPF 50+ with iron oxides, applied as final step. Tinted formulations provide built-in iron oxide protection. Apply ¼ teaspoon for face, allowing to set before makeup application.
Evening Recovery Protocol:
1. Thorough Cleanse: Remove all photoprotective products and environmental debris that could trigger overnight inflammation.
2. Gentle Exfoliation (2-3x weekly): Low-concentration AHA (5-8% glycolic or lactic acid) or PHA maintains even turnover without irritation. Skip if any signs of sensitivity present.
3. Treatment Actives: Retinoids (if tolerated) support cellular turnover and reduce UV-induced DNA damage. Alternative: azelaic acid 10-20% provides tyrosinase inhibition with anti-inflammatory benefits.
4. Barrier Repair: Richer moisturiser with ceramides, peptides, and antioxidants supports overnight recovery and barrier strengthening.
Seasonal Adjustments:
Australian summer (November-February) requires enhanced protection: SPF reapplication every 90-120 minutes during outdoor exposure, increased antioxidant concentration, heat avoidance strategies, and potential reduction of exfoliating actives to prevent irritation-triggered pigmentation.
Winter months (May-August) allow gentler introduction of treatment actives whilst maintaining daily photoprotection (UV Index still reaches 3-5, sufficient for pigmentation triggering in susceptible individuals).